Canada welcomes hundreds of thousands of immigrants and refugees every year. Many arrive with strength, resilience, and hope. What gets talked about far less is how quickly the mental health system can fall short of meeting their needs – and why that gap persists.
This article draws on published research and clinical experience to name the barriers that keep immigrants and refugees from getting mental health support in Canada. It’s worth reading whether you’re a newcomer yourself, whether you work with newcomers, or whether you simply care about a more fair and accessible mental health system.
What the Research Tells Us
Post-traumatic stress disorder, or PTSD, is a mental health condition that can develop after someone experiences or witnesses something deeply frightening or harmful. It can show up as flashbacks, nightmares, emotional numbness, difficulty sleeping, or a constant sense of danger. Many people living with PTSD don’t recognise it by that name – they just know something feels very wrong.
Despite those elevated rates, immigrants and refugees access mental health services at far lower rates than Canadian-born residents. A Statistics Canada study (Ng & Zhang, 2021) found that even when comparing people with similar levels of mental health, Canadian-born residents are significantly more likely to consult a mental health professional. Someone born here with average mental health is more likely to seek help than a newcomer who is struggling. The need is higher. The access is lower. That gap is what this article is about.
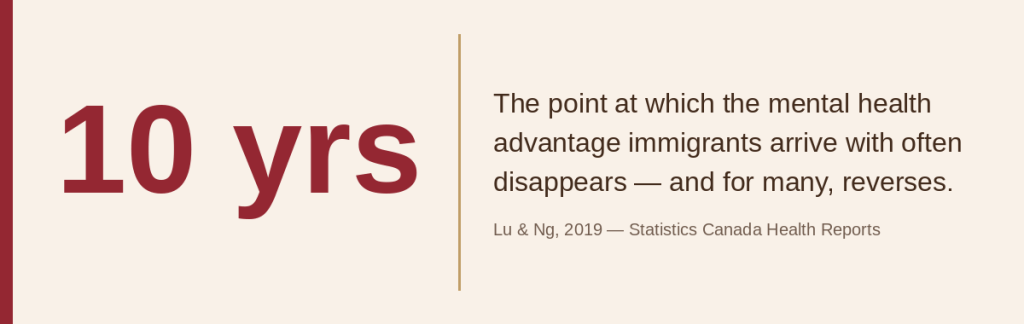
There’s another well-documented pattern worth understanding, often called the healthy immigrant effect. Immigrants arrive in Canada with better mental health than people born here – that’s well established in the research. But it fades.
What accounts for that shift? Years of unemployment or underemployment – working jobs far below your education level while professional credentials go unrecognised. Language barriers that don’t fully disappear. Being separated from family networks. Discrimination in workplaces and housing. The cumulative weight of those experiences, year after year, takes a real toll. This is confirmed across multiple Statistics Canada studies.
Refugees show this pattern most sharply. Statistics Canada data shows they report significantly more emotional difficulties and higher stress than family-class immigrants. Immigrants from South and Central America, North Africa, and parts of Asia experience more mental health struggles than those from Western Europe or the United States. That tracks closely with who faces the most discrimination and whose qualifications are least likely to be recognised here.
Trauma Doesn’t Stop at the Border
It’s easy to think of refugee trauma as something that happened before arrival – war, persecution, displacement, time in camps. That’s real. But the trauma often continues after people arrive.
Settlement itself can be traumatic. You’re learning how a new healthcare system works while trying to survive financially. You’re dealing with racism while looking for housing. You may be separated from family members for years while immigration paperwork moves slowly. You’re working multiple jobs and still can’t cover rent. This isn’t adjustment difficulty. For many people, it’s ongoing harm happening in real time.
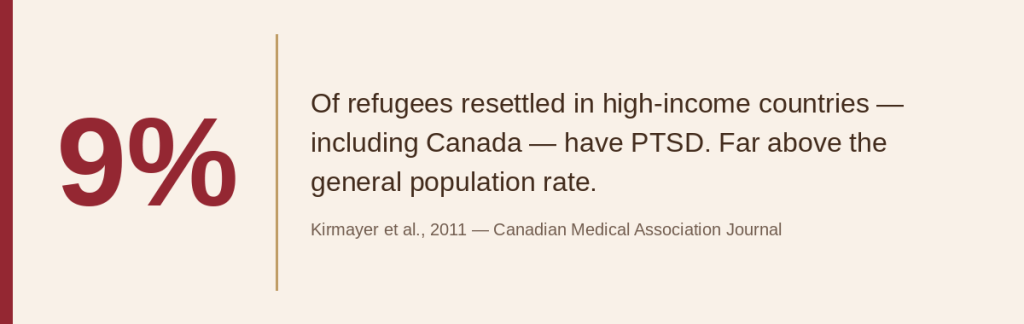
A study of Toronto Tamil refugees found that 12% met clinical criteria for PTSD – somewhat above the roughly 9% average seen across refugee populations resettled in developed countries, which is itself already high.
That gap between need and access is not a personal failure. It’s a system failure.
Seven Barriers That Keep People From Getting Help
These mental health barriers appear consistently across Canadian and international research. We’re naming them plainly because that’s the first step to doing something about them.
1. Mental health is understood differently across cultures
In many cultures, what Western psychiatry labels as a mental health condition is understood through different frameworks. Distress might be seen as a physical problem, a spiritual matter, a family concern, or a natural response to hard circumstances.
Some people describe emotional pain through physical symptoms because that’s how distress presents in their cultural context. Others see their struggles as tests of faith or character. Others believe healing happens in community, not in a one-on-one session with a stranger who has a degree. None of those frameworks are wrong. But they can make accessing Western-style mental health care feel foreign, or even unwelcoming.
2. The fear of stigma is rational, not just cultural
Stigma around mental health isn’t unique to immigrant communities. Plenty of Canadian-born people avoid therapy because of shame. But when you’re already managing racism, precarious immigration status, and community pressures, being seen as mentally unwell can add another layer of vulnerability.
In some communities, struggling with mental health can affect marriage prospects, family reputation, or standing in a religious community. For refugees, there’s sometimes a real fear that disclosing these struggles could affect immigration applications. For people with precarious status, there are genuine questions about what gets recorded and who has access to it.
The concern about privacy runs deeper than people might expect. We’ve had clients come to therapy without their partner or family knowing. In some cases, we only found out when asking about household income for our sliding scale fees. For some people – particularly women in households where seeking help carries stigma – that kind of secrecy is the only way they can access care. It’s a reminder that stigma isn’t only about what communities believe. It shapes what people feel safe doing.
Treating stigma as “something education alone can fix” misses the point. For many people, caution around the mental health system makes complete sense given their experiences. What helps is addressed later in this article.
3. Many people don’t know these services exist
In many countries, therapy is either unavailable, expensive, or only for people with severe psychiatric conditions. The idea that you can speak with a trained professional about stress, grief, or relationship struggles – and that this might be covered or subsidised – is not obvious if you’ve never lived somewhere that offered it.
Even when people know therapy exists in theory, they often don’t know where to find it, what the intake process looks like, or whether they would qualify. The Canadian healthcare system is confusing for people who grew up here. For someone navigating it for the first time, in a second or third language, figuring out how to access mental health support can feel impossible.
4. Language barriers go deeper than vocabulary
Language is a barrier – but it’s more complicated than whether someone speaks English.
Even when someone speaks English well, therapy asks you to put your most complex feelings into words in that language. Trauma has a mother tongue. Grief carries cultural meanings that don’t always translate cleanly. Some experiences simply don’t have equivalent words across languages.
It matters whether your therapist understands why something carries shame in your culture without needing a full explanation. It matters whether certain family dynamics make immediate sense to them. It matters whether you have to change how you speak and how you present yourself just to be understood.
Canada’s healthcare system doesn’t require interpretation services the way courts do, which means many people end up trying to discuss the most sensitive parts of their lives in their second or third language. That’s a significant gap in the system.
5. Trust has been broken by past experiences
Many racialized immigrants have experienced discrimination in Canadian healthcare – not as a rare exception, but as a pattern. Providers who rush through appointments. Clinicians who speak over someone because of an accent. Mental health professionals who treat normal cultural practices as symptoms. People being offered medication before they’ve had a chance to be heard.
This isn’t paranoia. When you’ve been dismissed or misunderstood repeatedly, you learn to be careful. You delay getting help. You don’t trust easily. That response makes sense.
Research shows that discrimination by healthcare providers adds directly to stress and discourages people from seeking support in the future. A 2016 report by the Mental Health Commission of Canada on refugee mental health found that systemic change – not just individual provider training – is needed to meaningfully address this pattern.
6. Practical barriers can make access impossible
Even when someone wants help, knows where to find it, and trusts the system enough to try, practical barriers can stop them entirely.
Cost is the obvious one. Many immigrants work jobs without benefits. Therapy in Ontario commonly runs $150 to $200 per session. If you’re sending money home or supporting family members through sponsorship, that’s not a realistic option.
But there are other barriers too. If you’re working multiple jobs, when do you go to therapy? Many low-wage workplaces don’t offer time off for medical appointments. Transportation costs money. Childcare costs money. If you’re in precarious housing, you may not even have a private space for an online session.
Research consistently identifies these structural obstacles – cost, transportation, and inflexible work schedules – as key reasons people don’t access care even when they want to.
At Cornerstone, we offer sliding scale fees based on household income and size, as well as affordable therapy with supervised interns. Residents of Peel Region who receive Ontario Works (OW) or Ontario Disability Support Program (ODSP) support may qualify for free counselling through our CARE grant program. We also offer online therapy with evening and Saturday morning hours to accommodate different work schedules.
7. Many providers aren’t equipped to help
This is hard to say, but it needs to be said: many mental health providers in Canada are not prepared to work effectively with immigrant and refugee populations.
Some don’t understand how cultural values shape family dynamics and decision-making. Some treat expected responses to trauma as clinical symptoms – like staying on high alert after surviving war, or feeling anxious when immigration status is uncertain. Some bring assumptions about how families should function or how people should express emotion.
Thomson et al. (2015), reviewing barriers to immigrant mental health access across Canada, described this as a gap in “provider attitudes and competence” – ranging from genuine cultural unfamiliarity to outright stereotyping. Either way, the result is the same: people don’t get the help they need, or they don’t come back.
What Actually Needs to Change
The common response to these barriers is to suggest cultural competency training or more translation services. Those things help. But they don’t fix the core problem: Canada’s mental health system was largely built for English-speaking people with stable employment and benefits. Newcomers are often navigating a system not designed with them in mind.
Asking people to become better at accessing a system that doesn’t work for them puts the burden in the wrong place. The system needs to change. That means:
- Community-embedded services – meeting people where they already go for support, rather than expecting them to navigate unfamiliar systems alone.
- Group and peer support programs – recognising that healing often happens in community, not just in individual therapy sessions.
- Economic supports – addressing the social conditions that drive poor mental health, not just treating the symptoms one person at a time.
- Access to professional interpretation in healthcare settings – courts require it; medical appointments should too.
- Anti-racism training that changes actual behaviour, not just awareness.
- Culturally adapted approaches that don’t force Western frameworks onto different understandings of distress.
For immigrants and refugees, settlement policy and mental health are inseparable. You can’t address depression in isolation from the social conditions someone is living in. Anxiety doesn’t exist in a vacuum when immigration status is precarious. The circumstances of people’s lives are not separate from their mental health – they’re central to it.
Why This Makes Us Better Therapists for Everyone
Learning to work across cultural difference makes you a better clinician, full stop.
When you stop assuming you know what a family should look like, you get better at not making assumptions about anyone. When you develop skills to work across language and cultural gaps, you become more attuned to all the ways people communicate pain. When you understand that trauma doesn’t follow a predictable timeline, you become a better trauma therapist regardless of who’s sitting across from you.
We call this cultural humility – staying curious, staying open, and following the client’s lead rather than imposing a framework. It’s not something we reserve for newcomer clients. It’s how we try to show up for everyone.
Great therapy happens across cultural lines all the time. What matters isn’t whether your therapist shares your exact background. It’s whether they bring genuine curiosity, real respect for your experience, and the skill to meet you where you are.
How Cornerstone Addresses These Barriers
Our team includes therapists born in Canada and those who came from somewhere else, some with personal immigration experiences. We offer counselling in English, French, and Arabic. We work to match clients with therapists who understand not just their language but their cultural context. Here is what we’ve built:
- Language access: Sessions available in English, French, and Arabic. We match clients with therapists who can work in their preferred language.
- Cultural understanding: Several of our therapists have personal immigration experiences. All are trained in culturally responsive, trauma-informed care.
- Affordable options: Sliding scale fees based on household income and size, plus affordable therapy with supervised interns. Peel Region residents on OW or ODSP may qualify for free counselling through our CARE grant.
- Community connections: We work with settlement agencies and organisations to reach newcomers who may not know counselling is available. Learn more about our Newcomer Services Office partnership.
- Children and youth: When parents are struggling, children often are too. Growing up between cultures carries its own pressures. We offer therapy for children and youth with therapists who understand those pressures.
- Flexible scheduling: Online therapy with evening and Saturday morning hours.
- Walk-in access: Our Rapid Access Counselling option means you don’t have to wait weeks for a first appointment.
We also offer free helpful mental health tools and curated video resources on our website.
If You’re Ready to Talk
If you’re in Ontario and struggling – whatever your background, whatever brought you here – we’re here when you’re ready.
You deserve care that respects your full story: your culture, your values, your experience, and what healing means to you. Whether you’re a newcomer or your family has been in Canada for generations, we work to meet you where you are.
To book your first appointment, visit cornerstonefamilycounselling.com/first-appointment, call us at 905.214.7363, or email [email protected].
A Note on Sources
The statistics in this article draw on peer-reviewed research and Statistics Canada data. A few points worth knowing:
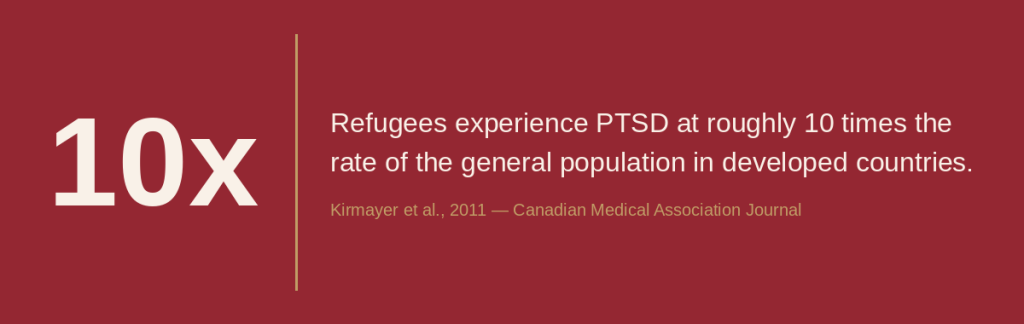
- The 10x PTSD figure for refugees is cited across multiple systematic reviews. The CMAJ paper by Kirmayer et al. (2011) provides a strong Canadian-focused synthesis.
- The 9% PTSD / 5% depression figures reflect ranges reported across studies of refugees resettled in high-income countries, consistent with the Kirmayer et al. (2011) summary.
- The healthy immigrant effect and its decline is supported by Statistics Canada’s Health Reports series, including Lu & Ng (2019).
- The finding that Canadian-born residents access mental health consultations at higher rates than newcomers comes from Ng & Zhang (2021) in Statistics Canada’s Health Reports.
- The Toronto Tamil refugee figure (12% PTSD, 1 in 10 receiving treatment) is cited within the Kirmayer et al. (2011) CMAJ paper.
- The “provider attitudes and competence” language comes from Thomson et al. (2015).
- Note on variation: Refugee mental health research covers diverse populations and methods. We have presented figures consistent with the consensus in the literature, not outliers.
References
Kirmayer, L. J., Narasiah, L., Munoz, M., Rashid, M., Ryder, A. G., Guzder, J., … & Pottie, K. (2011). Common mental health problems in immigrants and refugees: general approach in primary care. Canadian Medical Association Journal, 183(12), E959-E967.
Library of Parliament. (2022). Mental Health Needs of Refugees in Canada. HillNotes.
Lu, C., & Ng, E. (2019). Healthy immigrant effect by immigrant category in Canada. Health Reports, 30(4), 3-11. Statistics Canada.
Mental Health Commission of Canada. (2016). Supporting the Mental Health of Refugees to Canada. Ottawa.
Ng, E., & Zhang, H. (2021). Access to mental health consultations by immigrants and refugees in Canada. Health Reports, 32(6), 3-13. Statistics Canada.
Noh, S., Beiser, M., Kaspar, V., Hou, F., & Rummens, J. (1999). Perceived racial discrimination, depression and coping: A study of Southeast Asian refugees in Canada. Journal of Health and Social Behavior, 40(3), 193-207.
Salami, B., Yaskina, M., Hegadoren, K., et al. (2019). Access and utilization of mental health services for immigrants and refugees. International Journal of Mental Health Nursing, 28(1), 152-161.
Salam, Z., Carranza, M., Newbold, B., Wahoush, O., & Joseph, A. (2024). Racialized Immigrants’ Encounters of Barriers and Facilitators in Seeking Mental Healthcare Services in Ontario, Canada. Community Mental Health Journal.
Thomson, M. S., Chaze, F., George, U., & Guruge, S. (2015). Improving immigrant populations’ access to mental health services in Canada: A review of barriers and recommendations. Journal of Immigrant and Minority Health, 17(6), 1895-1905.